What Is The Big Cause Of Achilles Tendon Pain ?
Overview
 This nagging injury can be long-lasting if not treated - and if your running form needs some work. The name Achilles is said to be a combination of two Greek words that together mean ?grief of the people.? The injury that bears that hero?s name, in honor of his only weakness, certainly aggrieves many runners, with Achilles tendinitis accounting for around 10 percent of running injuries. Technically, Achilles tendinitis is acute inflammation of the tendon that runs along the back of the ankle. Pain in that area for longer than a couple weeks is not really tendinitis anymore. Athletes, however, tend to characterize any pain along the tendon above the back of the heel as Achilles tendinitis. Achilles tendinitis can be confused with other injuries, such as heel problems, but the hallmark sign is if you?re pinching the Achilles and it?s really sore.
This nagging injury can be long-lasting if not treated - and if your running form needs some work. The name Achilles is said to be a combination of two Greek words that together mean ?grief of the people.? The injury that bears that hero?s name, in honor of his only weakness, certainly aggrieves many runners, with Achilles tendinitis accounting for around 10 percent of running injuries. Technically, Achilles tendinitis is acute inflammation of the tendon that runs along the back of the ankle. Pain in that area for longer than a couple weeks is not really tendinitis anymore. Athletes, however, tend to characterize any pain along the tendon above the back of the heel as Achilles tendinitis. Achilles tendinitis can be confused with other injuries, such as heel problems, but the hallmark sign is if you?re pinching the Achilles and it?s really sore.
Causes
Hill running or stair climbing. Overuse resulting from the natural lack of flexibility in the calf muscles. Rapidly increasing mileage or speed. Starting up too quickly after a layoff. Trauma caused by sudden and hard contraction of the calf muscles when putting out extra effort such as in a final sprint. Achilles tendinitis often begins with mild pain after exercise or running that gradually worsens.
Symptoms
People with Achilles tendinitis may experience pain during and after exercising. Running and jumping activities become painful and difficult. Symptoms include stiffness and pain in the back of the ankle when pushing off the ball of the foot. For patients with chronic tendinitis (longer than six weeks), x-rays may reveal calcification (hardening of the tissue) in the tendon. Chronic tendinitis can result in a breakdown of the tendon, or tendinosis, which weakens the tendon and may cause a rupture.
Diagnosis
A podiatrist can usually make the diagnosis by clinical history and physical examination alone. Pain with touching or stretching the tendon is typical. There may also be a visible swelling to the tendon. The patient frequently has difficulty plantarflexing (pushing down the ball of the foot and toes, like one would press on a gas pedal), particularly against resistance. In most cases X-rays don't show much, as they tend to show bone more than soft tissues. But X-rays may show associated degeneration of the heel bone that is common with Achilles Tendon problems. For example, heel spurs, calcification within the tendon, avulsion fractures, periostitis (a bruising of the outer covering of the bone) may all be seen on X-ray. In cases where we are uncertain as to the extent of the damage to the tendon, though, an MRI scan may be necessary, which images the soft tissues better than X-rays. When the tendon is simply inflamed and not severely damaged, the problem may or may not be visible on MRI. It depends upon the severity of the condition.
Nonsurgical Treatment
Treatment will focus on relieving the pain and preventing further injury. Your podiatrist may create shoe inserts or a soft cast to effectively immobilize the affected area for a period of time. (Often, a couple of weeks are needed for the tendon to heal.) Medication can help too. Your podiatrist may recommend or prescribe oral medication.

Surgical Treatment
Many people don't realize that Achilles tendon surgery can be very traumatic to your body. The type of trauma you experience after surgery can be compared to what you go through when you first injured your Achilles tendon. During the first 24 to 72 hours after the surgery your ankle will be tender, swollen and very painful. Your leg will be weak and unstable making it impossible for you to put weight on your leg without some kind of help. This is why your doctor or surgeon will have you outfitted for a cast, ankle brace and/or crutches before the procedure. When you are relying on a cast/brace and crutches your Achilles tendon is less likely to be as active as it once was. This is usually why atrophy (loss) of your lower leg muscles (specifically your calf muscle) happens. In general, more than 80%* of people who undergo surgery for an injured Achilles Tendon are able to return to their active lifestyle. In order to avoid re-injury, it is important to commit to a regular conservative therapy routine.
Prevention
While it may not be possible to prevent Achilles tendinitis, you can take measures to reduce your risk. Increase your activity level gradually. If you're just beginning an exercise regimen, start slowly and gradually increase the duration and intensity of the training. Take it easy. Avoid activities that place excessive stress on your tendons, such as hill running. If you participate in a strenuous activity, warm up first by exercising at a slower pace. If you notice pain during a particular exercise, stop and rest. Choose your shoes carefully. The shoes you wear while exercising should provide adequate cushioning for your heel and should have a firm arch support to help reduce the tension in the Achilles tendon. Replace your worn-out shoes. If your shoes are in good condition but don't support your feet, try arch supports in both shoes. Stretch daily. Take the time to stretch your calf muscles and Achilles tendon in the morning, before exercise and after exercise to maintain flexibility. This is especially important to avoid a recurrence of Achilles tendinitis. Strengthen your calf muscles. Strong calf muscles enable the calf and Achilles tendon to better handle the stresses they encounter with activity and exercise. Cross-train. Alternate high-impact activities, such as running and jumping, with low-impact activities, such as cycling and swimming.
This nagging injury can be long-lasting if not treated - and if your running form needs some work. The name Achilles is said to be a combination of two Greek words that together mean ?grief of the people.? The injury that bears that hero?s name, in honor of his only weakness, certainly aggrieves many runners, with Achilles tendinitis accounting for around 10 percent of running injuries. Technically, Achilles tendinitis is acute inflammation of the tendon that runs along the back of the ankle. Pain in that area for longer than a couple weeks is not really tendinitis anymore. Athletes, however, tend to characterize any pain along the tendon above the back of the heel as Achilles tendinitis. Achilles tendinitis can be confused with other injuries, such as heel problems, but the hallmark sign is if you?re pinching the Achilles and it?s really sore.
Causes
Hill running or stair climbing. Overuse resulting from the natural lack of flexibility in the calf muscles. Rapidly increasing mileage or speed. Starting up too quickly after a layoff. Trauma caused by sudden and hard contraction of the calf muscles when putting out extra effort such as in a final sprint. Achilles tendinitis often begins with mild pain after exercise or running that gradually worsens.
Symptoms
People with Achilles tendinitis may experience pain during and after exercising. Running and jumping activities become painful and difficult. Symptoms include stiffness and pain in the back of the ankle when pushing off the ball of the foot. For patients with chronic tendinitis (longer than six weeks), x-rays may reveal calcification (hardening of the tissue) in the tendon. Chronic tendinitis can result in a breakdown of the tendon, or tendinosis, which weakens the tendon and may cause a rupture.
Diagnosis
A podiatrist can usually make the diagnosis by clinical history and physical examination alone. Pain with touching or stretching the tendon is typical. There may also be a visible swelling to the tendon. The patient frequently has difficulty plantarflexing (pushing down the ball of the foot and toes, like one would press on a gas pedal), particularly against resistance. In most cases X-rays don't show much, as they tend to show bone more than soft tissues. But X-rays may show associated degeneration of the heel bone that is common with Achilles Tendon problems. For example, heel spurs, calcification within the tendon, avulsion fractures, periostitis (a bruising of the outer covering of the bone) may all be seen on X-ray. In cases where we are uncertain as to the extent of the damage to the tendon, though, an MRI scan may be necessary, which images the soft tissues better than X-rays. When the tendon is simply inflamed and not severely damaged, the problem may or may not be visible on MRI. It depends upon the severity of the condition.
Nonsurgical Treatment
Treatment will focus on relieving the pain and preventing further injury. Your podiatrist may create shoe inserts or a soft cast to effectively immobilize the affected area for a period of time. (Often, a couple of weeks are needed for the tendon to heal.) Medication can help too. Your podiatrist may recommend or prescribe oral medication.
Surgical Treatment
Many people don't realize that Achilles tendon surgery can be very traumatic to your body. The type of trauma you experience after surgery can be compared to what you go through when you first injured your Achilles tendon. During the first 24 to 72 hours after the surgery your ankle will be tender, swollen and very painful. Your leg will be weak and unstable making it impossible for you to put weight on your leg without some kind of help. This is why your doctor or surgeon will have you outfitted for a cast, ankle brace and/or crutches before the procedure. When you are relying on a cast/brace and crutches your Achilles tendon is less likely to be as active as it once was. This is usually why atrophy (loss) of your lower leg muscles (specifically your calf muscle) happens. In general, more than 80%* of people who undergo surgery for an injured Achilles Tendon are able to return to their active lifestyle. In order to avoid re-injury, it is important to commit to a regular conservative therapy routine.
Prevention
While it may not be possible to prevent Achilles tendinitis, you can take measures to reduce your risk. Increase your activity level gradually. If you're just beginning an exercise regimen, start slowly and gradually increase the duration and intensity of the training. Take it easy. Avoid activities that place excessive stress on your tendons, such as hill running. If you participate in a strenuous activity, warm up first by exercising at a slower pace. If you notice pain during a particular exercise, stop and rest. Choose your shoes carefully. The shoes you wear while exercising should provide adequate cushioning for your heel and should have a firm arch support to help reduce the tension in the Achilles tendon. Replace your worn-out shoes. If your shoes are in good condition but don't support your feet, try arch supports in both shoes. Stretch daily. Take the time to stretch your calf muscles and Achilles tendon in the morning, before exercise and after exercise to maintain flexibility. This is especially important to avoid a recurrence of Achilles tendinitis. Strengthen your calf muscles. Strong calf muscles enable the calf and Achilles tendon to better handle the stresses they encounter with activity and exercise. Cross-train. Alternate high-impact activities, such as running and jumping, with low-impact activities, such as cycling and swimming.
What Is Painful Heel And Best Ways To Fix It

Overview
The plantar fascia is a thickened fibrous aponeurosis that originates from the medial tubercle of the calcaneus, runs forward to insert into the deep, short transverse ligaments of the metatarsal heads, dividing into 5 digital bands at the metatarsophalangeal joints and continuing forward to form the fibrous flexor sheathes on the plantar aspect of the toes. Small plantar nerves are invested in and around the plantar fascia, acting to register and mediate pain.
Causes
You're more likely to develop the condition if you're female, overweight or have a job that requires a lot of walking or standing on hard surfaces. You're also at risk if you walk or run for exercise, especially if you have tight calf muscles that limit how far you can flex your ankles. People with very flat feet or very high arches also are more prone to plantar fasciitis.
Symptoms
Most people with plantar fasciitis have pain when they take their first steps after they get out of bed or sit for a long time. You may have less stiffness and pain after you take a few steps. But your foot may hurt more as the day goes on. It may hurt the most when you climb stairs or after you stand for a long time. If you have foot pain at night, you may have a different problem, such as arthritis , or a nerve problem such as tarsal tunnel syndrome.
Diagnosis
Your doctor can usually diagnose plantar fasciitis just by talking to you and examining your feet. Rarely, tests are needed if the diagnosis is uncertain or to rule out other possible causes of heel pain. These can include X-rays of the heel or an ultrasound scan of the fascia. An ultrasound scan usually shows thickening and swelling of the fascia in plantar fasciitis.
Non Surgical Treatment
Over-the-counter Orthotics. A soft, over-the-counter orthotic (Prefabricated orthotic) with an accommodating arch support has proven to be quite helpful in the management of plantar fascia symptoms. Studies demonstrate that it is NOT necessary to obtain a custom orthotic for the treatment of this problem. Comfort Shoes. Shoes with a stiff sole, rocker-bottom contour, and a comfortable leather upper combined with an over-the-counter orthotic or a padded heel can be very helpful in the treatment of plantar fasciitis. Anti-Inflammatory Medication (NSAIDs): A short course of over-the-counter anti-inflammatory medications may be helpful in managing plantar fasciitis symptoms providing the patient does not have any contra-indications such as a history of stomach ulcers. Activity Modification Any activity that has recently been started, such as a new running routine or a new exercise at the gym that may have increased loading through the heel area, should be stopped on a temporary basis until the symptoms have resolved. At that point, these activities can be gradually started again. Also, any activity changes (ex. sitting more) that will limit the amount of time a patient is on their feet each day may be helpful. A night splint, which keeps the ankle in a neutral position (right angle) while the patient sleeps, can be very helpful in alleviating the significant morning symptoms. A night splint may be prescribed by your physician. Alternatively, it can be ordered online or even obtained in some medical supply stores. This splint is worn nightly for 1-3 weeks until the cycle of pain is broken. Furthermore, this splinting can be reinstituted for a short period of time is symptoms recur.

Surgical Treatment
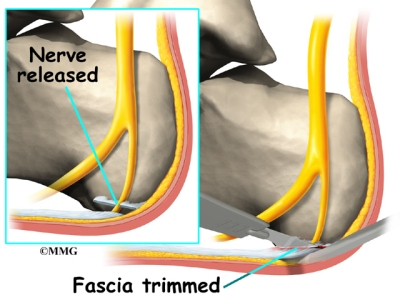
The most common surgical procedure for plantar fasciitis is plantar fascia release. It involves surgical removal of a part from the plantar fascia ligament which will relieve the inflammation and reduce the tension. Plantar fascia release is either an open surgery or endoscopic surgery (insertion of special surgical instruments through small incisions). While both methods are performed under local anesthesia the open procedure may take more time to recover. Other surgical procedures can be used as well but they are rarely an option. Complications of plantar fasciitis surgery are rare but they are not impossible. All types of plantar fasciitis surgery pose a risk of infection, nerve damage, and anesthesia related complications including systemic toxicity, and persistence or worsening of heel pain.
What Causes Pain Of The Heel And The Way To Heal It

Overview
If you experience sharp, throbbing or aching heel pain with your first steps out of bed each morning, or when walking throughout the day, you may be suffering from Plantar Fasciitis. This guide will help you to understand the definition, symptoms and causes of this condition and will explore your treatment options for rapid relief from your pain.
Causes
A number of factors can contribute to plantar fasciitis. While men can get plantar fasciitis, it is more common in women. You're also more likely to have this condition as you age or if you are overweight. Take up a new form of exercise or suddenly increase the intensity of your exercise. Are on your feet for several hours each day. Have other medical conditions such as rheumatoid arthritis or lupus (systemic lupus erythematosus). Tend to wear high-heeled shoes, and then switch abruptly to flat shoes. Wear shoes that are worn out with weak arch supports and thin soles. Have flat feet or an unusually high arch. Have legs of uneven lengths or an abnormal walk or foot position. Have tight achilles tendons, or ‘heel cords’.
Symptoms
The classic sign of plantar fasciitis is that the worst pain occurs with the first few steps in the morning, but not every patient will have this symptom. Patients often notice pain at the beginning of activity that lessens or resolves as they warm up. The pain may also occur with prolonged standing and is sometimes accompanied by stiffness. In more severe cases, the pain will also worsen toward the end of the day.
Diagnosis
Your doctor can usually diagnose plantar fasciitis just by talking to you and examining your feet. Rarely, tests are needed if the diagnosis is uncertain or to rule out other possible causes of heel pain. These can include X-rays of the heel or an ultrasound scan of the fascia. An ultrasound scan usually shows thickening and swelling of the fascia in plantar fasciitis.
Non Surgical Treatment
There are several things you can do to self-treat your heel or arch pain. The first thing is to wear better shoes and consider adding arch supports or custom foot orthotics to your shoes. Stretching the calf muscles can also often be helpful. Try to stretch when you first get up in the morning and before you go to bed at night. Another good exercise is to "roll" your arch and heel. This is done by placing a tennis ball, golf ball, or lacrosse ball on the floor and rolling your foot on top of it. Some people get extra benefit by "rolling" on a frozen water bottle. You should also carefully evaluate your fitness program as you may be overdoing it. You may want consider backing of new or recently added exercises or increases in training until your heel pain improves. If you work at a standing job try to take more time to walk around during the day and avoid standing in one place for too long.

Surgical Treatment
Although most patients with plantar fasciitis respond to non-surgical treatment, a small percentage of patients may require surgery. If, after several months of non-surgical treatment, you continue to have heel pain, surgery will be considered. Your foot and ankle surgeon will discuss the surgical options with you and determine which approach would be most beneficial for you. No matter what kind of treatment you undergo for plantar fasciitis, the underlying causes that led to this condition may remain. Therefore, you will need to continue with preventive measures. Wearing supportive shoes, stretching, and using custom orthotic devices are the mainstay of long-term treatment for plantar fasciitis.
What Triggers Painful Heel To Flare Up

Overview
Plantar fasciitis refers to an inflammation of the plantar fascia, a thick, fibrous band running along the sole of the foot. Such inflammation results from direct injury to the plantar fascia, usually, repeated trauma to the tissue where the fascia attaches to the calcaneus or heel bone. The plantar fascia is critical in maintaining the foot’s complex arch system, also playing a role in balance and fine control of certain phases of the athlete’s gait. Injury to the plantar fascia is particularly painful and disabling for runners and can often prove stubbornly resistant to treatment. Rehabilitation is frequently a lengthy and frustrating process. For these reasons, care should be taken where possible to avoid such injury by means of preventative exercises and sensitivity to early warning signs.
Causes
A variety of causes exist for plantar fasciitis. Some of the most common causes include excessive weight load on the foot due to obesity or prolonged standing, mechanical imbalances of the foot, osteoarthritis and rheumatoid arthritis, sudden increase in body weight (e.g., pregnancy), sudden increase in walking or running, tight calf muscles is a very common cause of the disorder, wearing shoes with poor support, including flip-flops. Another cause of pain is the shortening of the plantar fascia overnight due to the ankle bending, causing the toes to point towards the ground. The plantar fascia stretches in the morning when you stand. The act of lengthening it causes a great deal of pain. However, this is not limited to an overnight occurrence, it can happen any time the foot is flexed (i.e., pointed) for extended periods of time. For example, driving in the car for long periods can cause fasciitis in the right foot, which steps on the accelerator.
Symptoms
Plantar fasciitis generally occurs in one foot. Bilateral plantar fasciitis is unusual and tends to be the result of a systemic arthritic condition that is exceptionally rare among athletes. Males suffer from a somewhat greater incidence of plantar fasciitis than females, perhaps as a result of greater weight coupled with greater speed and ground impact, as well as less flexibility in the foot. Typically, the sufferer of plantar fasciitis experiences pain upon rising after sleep, particularly the first step out of bed. Such pain is tightly localized at the bony landmark on the anterior medial tubercle of the calcaneus. In some cases, pain may prevent the athlete from walking in a normal heel-toe gait, causing an irregular walk as means of compensation. Less common areas of pain include the forefoot, Achilles tendon, or subtalar joint. After a brief period of walking, the pain usually subsides, but returns again either with vigorous activity or prolonged standing or walking. On the field, an altered gait or abnormal stride pattern, along with pain during running or jumping activities are tell-tale signs of plantar fasciitis and should be given prompt attention. Further indications of the injury include poor dorsiflexion (lifting the forefoot off the ground) due to a shortened gastroc complex, (muscles of the calf). Crouching in a full squat position with the sole of the foot flat on the ground can be used as a test, as pain will preclude it for the athlete suffering from plantar fasciitis, causing an elevation of the heel due to tension in the gastroc complex.
Diagnosis
Plantar fasciitis is usually diagnosed by a health care provider after consideration of a person’s presenting history, risk factors, and clinical examination. Tenderness to palpation along the inner aspect of the heel bone on the sole of the foot may be elicited during the physical examination. The foot may have limited dorsiflexion due to tightness of the calf muscles or the Achilles tendon. Dorsiflexion of the foot may elicit the pain due to stretching of the plantar fascia with this motion. Diagnostic imaging studies are not usually needed to diagnose plantar fasciitis. However, in certain cases a physician may decide imaging studies (such as X-rays, diagnostic ultrasound or MRI) are warranted to rule out other serious causes of foot pain. Bilateral heel pain or heel pain in the context of a systemic illness may indicate a need for a more in-depth diagnostic investigation. Lateral view x-rays of the ankle are the recommended first-line imaging modality to assess for other causes of heel pain such as stress fractures or bone spur development. Plantar fascia aponeurosis thickening at the heel greater than 5 millimeters as demonstrated by ultrasound is consistent with a diagnosis of plantar fasciitis. An incidental finding associated with this condition is a heel spur, a small bony calcification on the calcaneus (heel bone), which can be found in up to 50% of those with plantar fasciitis. In such cases, it is the underlying plantar fasciitis that produces the heel pain, and not the spur itself. The condition is responsible for the creation of the spur though the clinical significance of heel spurs in plantar fasciitis remains unclear.
Non Surgical Treatment
No single treatment works best for everyone with plantar fasciitis. But there are many things you can try to help your foot get better. Give your feet a rest. Cut back on activities that make your foot hurt. Try not to walk or run on hard surfaces. To reduce pain and swelling, try putting ice on your heel. Or take an over-the-counter pain reliever like ibuprofen (such as Advil or Motrin) or naproxen (such as Aleve). Do toe stretches , calf stretches and towel stretches several times a day, especially when you first get up in the morning. (For towel stretches, you pull on both ends of a rolled towel that you place under the ball of your foot.) Get a new pair of shoes. Pick shoes with good arch support and a cushioned sole. Or try heel cups or shoe inserts ( orthotics ). Use them in both shoes, even if only one foot hurts. If these treatments do not help, your doctor may recommend splints that you wear at night, shots of medicine (such as a steroid ) in your heel, or other treatments. You probably will not need surgery. Doctors only suggest it for people who still have pain after trying other treatments for 6 to 12 months.

Surgical Treatment
Most studies indicate that 95% of those afflicted with plantar fasciitis are able to relieve their heel pain with nonsurgical treatments. If you are one of the few people whose symptoms don't improve with other treatments, your doctor may recommend plantar fascia release surgery. Plantar fascia release involves cutting part of the plantar fascia ligament in order to release the tension and relieve the inflammation of the ligament. Overall, the success rate of surgical release is 70 to 90 percent in patients with plantar fasciitis. While the success rate is very high following surgery, one should be aware that there is often a prolonged postoperative period of discomfort similar to the discomfort experienced prior to surgery. This pain usually will abate within 2-3 months. One should always be sure to understand all the risks associated with any surgery they are considering.
Prevention
Preventing plantar fasciitis is crucial. There are many choices to help prevent the occurrence of this condition, and keep it from returning. One of the most important is maintaining a healthy weight in order to reduce tension on the plantar fascia. In addition, shoes are very important, and should fit well and provide ample cushioning and support throughout the heel, arch, and ball of the foot so that weight is distributed evenly throughout the foot. Try to avoid walking barefoot on hard surfaces and replace old shoes before they wear out, especially shoes that you run or exercise in. When exercising, start off slow and ease into new routines to prevent sudden or excessive stress on tissue. Lastly, keep your calf muscles and the tissue of your feet stretched. Greater flexibility in the tissue makes them less susceptible to damage.
What Causes Pain On The Heel And Ways To Heal It

Overview
The plantar fascia is a thickened fibrous aponeurosis that originates from the medial tubercle of the calcaneus, runs forward to insert into the deep, short transverse ligaments of the metatarsal heads, dividing into 5 digital bands at the metatarsophalangeal joints and continuing forward to form the fibrous flexor sheathes on the plantar aspect of the toes. Small plantar nerves are invested in and around the plantar fascia, acting to register and mediate pain.
Causes
Identified risk factors for plantar fasciitis include excessive running, standing on hard surfaces for prolonged periods of time, high arches of the feet, the presence of a leg length inequality, and flat feet. The tendency of flat feet to excessively roll inward during walking or running makes them more susceptible to plantar fasciitis. Obesity is seen in 70% of individuals who present with plantar fasciitis and is an independent risk factor. Studies have suggested a strong association exists between an increased body mass index and the development of plantar fasciitis. Achilles tendon tightness and inappropriate footwear have also been identified as significant risk factors.
Symptoms
Plantar fasciosis is characterized by pain at the bottom of the heel with weight bearing, particularly when first arising in the morning; pain usually abates within 5 to 10 min, only to return later in the day. It is often worse when pushing off of the heel (the propulsive phase of gait) and after periods of rest. Acute, severe heel pain, especially with mild local puffiness, may indicate an acute fascial tear. Some patients describe burning or sticking pain along the plantar medial border of the foot when walking.
Diagnosis
Your doctor will check your feet and watch you stand and walk. He or she will also ask questions about your past health, including what illnesses or injuries you have had. Your symptoms, such as where the pain is and what time of day your foot hurts most. How active you are and what types of physical activity you do. Your doctor may take an X-ray of your foot if he or she suspects a problem with the bones of your foot, such as a stress fracture.
Non Surgical Treatment
In the early stages of plantar fasciitis resting the foot may ease the pain. Medication to reduce inflammation should help but should only be used short term. Strapping may temporarily reduce the pain. All of the above therapies are only temporary measures and the pain is likely to reoccur if the cause of the abnormal pressure which has triggered the plantar fasciitis has not been identified. In order to establish the cause of the plantar fasciitis a biomechanical assessment may be required.
Surgical Treatment
Surgery is usually not needed for plantar fasciitis. About 95 out of 100 people who have plantar fasciitis are able to relieve heel pain without surgery. Your doctor may consider surgery if non-surgical treatment has not helped and heel pain is restricting your daily activities. Some doctors feel that you should try non-surgical treatment for at least 6 months before you consider surgery. The main types of surgery for plantar fasciitis are Plantar fascia release. This procedure involves cutting part of the plantar fascia ligament . This releases the tension on the ligament and relieves inflammation . Other procedures, such as removing a heel spur or stretching or loosening specific foot nerves. These surgeries are usually done in combination with plantar fascia release when there is lasting heel pain and another heel problem. Experts in the past thought that heel spurs caused plantar fasciitis. Now experts generally believe that heel spurs are the result, not the cause, of plantar fasciitis. Many people with large heel spurs never have heel pain or plantar fasciitis. So surgery to remove heel spurs is rarely done.
Symptoms Of Equinus
The causes of lip swelling could range from trauma and contact dermatitis to allergic reactions to certain medical conditions. I am a 44 year old Pe teacher who has been experiencing Claw Toe since October. Vinegar has been used as a condiment for several centuries.
These conditions include different types of arthritis , osteonecrosis , neuromas , tumors, or infections. Lastly, traumatic injuries, including fractures and ligament tears, can cause this type of foot pain. Treatment of foot pain often consists of anti-inflammatory medications , footwear modifications, and inserts for your shoes. When buying footwear, look for shoes with a wide toebox, good support, and avoid high heels. These pads help to take pressure off the ball of the foot. If some simple steps do not alleviate your symptoms, you should see your doctor to ensure you are receiving adequate treatment. In some rare situations, patients don't find relief with shoe modifications, and may require a surgical procedure. Remember that our shoes protect us from injury.
Most flat feet usually do not cause pain or other problems. Flat feet may be associated with pronation, a leaning inward of the ankle bones toward the center line. Foot pain, ankle pain or lower leg pain, especially in children, may be a result of flat feet and should be evaluated.
Rheumatoid arthritis causes forefoot deformity and often may cause displacement and even dislocation of the metatarsal joints themselves. Morton's Neuroma can also be a source of metarsalgia and is characterized by pain in the forefoot. Sesamoiditis is located on the plantar surface of the foot and will be located near the first metatarsal phalangeal joint.
The ezWalker® Custom Performance Insole can help relieve the pain and pressure of hammer toe by strategically supporting the medial, lateral, and trans-metatarsal arches to relieve pressure on the ball of the foot and therefore, release the action causing the hammer toe in the first place. Each ezWalker Performance Insole is custom molded to the specifications of each one of your feet, providing you with the support and comfort you need to relieve pain and produce comfort. Whether your hammer toe condition is due to genetics or not, ezWalker® Custom Performance Insoles can help you find relief from hammer toe and foot pain. The back of your ankle may feel tight and sore.
These conditions include different types of arthritis , osteonecrosis , neuromas , tumors, or infections. Lastly, traumatic injuries, including fractures and ligament tears, can cause this type of foot pain. Treatment of foot pain often consists of anti-inflammatory medications , footwear modifications, and inserts for your shoes. When buying footwear, look for shoes with a wide toebox, good support, and avoid high heels. These pads help to take pressure off the ball of the foot. If some simple steps do not alleviate your symptoms, you should see your doctor to ensure you are receiving adequate treatment. In some rare situations, patients don't find relief with shoe modifications, and may require a surgical procedure. Remember that our shoes protect us from injury.
Most flat feet usually do not cause pain or other problems. Flat feet may be associated with pronation, a leaning inward of the ankle bones toward the center line. Foot pain, ankle pain or lower leg pain, especially in children, may be a result of flat feet and should be evaluated.
Rheumatoid arthritis causes forefoot deformity and often may cause displacement and even dislocation of the metatarsal joints themselves. Morton's Neuroma can also be a source of metarsalgia and is characterized by pain in the forefoot. Sesamoiditis is located on the plantar surface of the foot and will be located near the first metatarsal phalangeal joint.
The ezWalker® Custom Performance Insole can help relieve the pain and pressure of hammer toe by strategically supporting the medial, lateral, and trans-metatarsal arches to relieve pressure on the ball of the foot and therefore, release the action causing the hammer toe in the first place. Each ezWalker Performance Insole is custom molded to the specifications of each one of your feet, providing you with the support and comfort you need to relieve pain and produce comfort. Whether your hammer toe condition is due to genetics or not, ezWalker® Custom Performance Insoles can help you find relief from hammer toe and foot pain. The back of your ankle may feel tight and sore.
Achilles Tendinitis
Overview
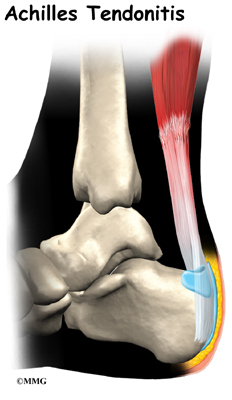 Achilles tendinitis is an inflammation (swelling) of the tendon, which usually occurs as a result of overuse injury. Basketball players are the most susceptible to Achilles tendinitis because of the frequent jumping. Any activity requiring a constant pushing off the foot, such as running or dancing, may result in swelling of the tendon.
Achilles tendinitis is an inflammation (swelling) of the tendon, which usually occurs as a result of overuse injury. Basketball players are the most susceptible to Achilles tendinitis because of the frequent jumping. Any activity requiring a constant pushing off the foot, such as running or dancing, may result in swelling of the tendon.
Causes
Poorly conditioned athletes are at the highest risk for developing Achilles tendonitis, also sometimes called Achilles tendinitis. Participating in activities that involve sudden stops and starts and repetitive jumping (e.g., basketball, tennis, dancing) increases the risk for the condition. It often develops following sudden changes in activity level, training on poor surfaces, or wearing inappropriate footwear. Achilles tendonitis may be caused by a single incident of overstressing the tendon, or it may result from a series of stresses that produce small tears over time (overuse). Patients who develop arthritis in the heel have an increased risk for developing Achilles tendonitis. This occurs more often in people who middle aged and older. The condition also may develop in people who exercise infrequently and in those who are just beginning an exercise program, because inactive muscles and tendons have little flexibility because of inactivity. It is important for people who are just starting to exercise to stretch properly, start slowly, and increase gradually. In some cases, a congenital (i.e., present at birth) condition causes Achilles tendonitis. Typically, this is due to abnormal rotation of the foot and leg (pronation), which causes the arch of the foot to flatten and the leg to twist more than normal.
Symptoms
Common symptoms of Achilles tendinitis include weakness in the leg, slight pain above the heel in the lower leg after activity, feeling of stiffness in the leg that usually appears in the morning and lessens throughout the day, bad pain the day after exercising, pain as you climb stairs or go uphill, swelling in the area of the Achilles tendon, creaking or cracking noise when you press on the Achilles tendon.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
In most cases, nonsurgical treatment options will provide pain relief, although it may take a few months for symptoms to completely subside. Even with early treatment, the pain may last longer than 3 months. If you have had pain for several months before seeking treatment, it may take 6 months before treatment methods take effect. The first step in reducing pain is to decrease or even stop the activities that make the pain worse. If you regularly do high-impact exercises (such as running), switching to low-impact activities will put less stress on the Achilles tendon. Cross-training activities such as biking, elliptical exercise, and swimming are low-impact options to help you stay active. Placing ice on the most painful area of the Achilles tendon is helpful and can be done as needed throughout the day. This can be done for up to 20 minutes and should be stopped earlier if the skin becomes numb. A foam cup filled with water and then frozen creates a simple, reusable ice pack. After the water has frozen in the cup, tear off the rim of the cup. Then rub the ice on the Achilles tendon. With repeated use, a groove that fits the Achilles tendon will appear, creating a "custom-fit" ice pack. Drugs such as ibuprofen and naproxen reduce pain and swelling. They do not, however, reduce the thickening of the degenerated tendon. Using the medication for more than 1 month should be reviewed with your primary care doctor. The following exercise can help to strengthen the calf muscles and reduce stress on the Achilles tendon. Lean forward against a wall with one knee straight and the heel on the ground. Place the other leg in front, with the knee bent. To stretch the calf muscles and the heel cord, push your hips toward the wall in a controlled fashion. Hold the position for 10 seconds and relax. Repeat this exercise 20 times for each foot. A strong pull in the calf should be felt during the stretch. Physical therapy is very helpful in treating Achilles tendinitis. It has proven to work better for noninsertional tendinitis than for insertional tendinitis. Eccentric strengthening is defined as contracting (tightening) a muscle while it is getting longer. Eccentric strengthening exercises can cause damage to the Achilles tendon if they are not done correctly. At first, they should be performed under the supervision of a physical therapist. Once mastered with a therapist, the exercises can then be done at home. These exercises may cause some discomfort, however, it should not be unbearable. Stand at the edge of a stair, or a raised platform that is stable, with just the front half of your foot on the stair. This position will allow your heel to move up and down without hitting the stair. Care must be taken to ensure that you are balanced correctly to prevent falling and injury. Be sure to hold onto a railing to help you balance. Lift your heels off the ground then slowly lower your heels to the lowest point possible. Repeat this step 20 times. This exercise should be done in a slow, controlled fashion. Rapid movement can create the risk of damage to the tendon. As the pain improves, you can increase the difficulty level of the exercise by holding a small weight in each hand. This exercise is performed similarly to the bilateral heel drop, except that all your weight is focused on one leg. This should be done only after the bilateral heel drop has been mastered. Cortisone, a type of steroid, is a powerful anti-inflammatory medication. Cortisone injections into the Achilles tendon are rarely recommended because they can cause the tendon to rupture (tear).

Surgical Treatment
For paratenonitis, a technique called brisement is an option. Local anesthetic is injected into the space between the tendon and its surrounding sheath to break up scar tissue. This can be beneficial in earlier stages of the problem 30 to 50 percent of the time, but may need to be repeated two to three times. Surgery consists of cutting out the surrounding thickened and scarred sheath. The tendon itself is also explored and any split tears within the tendon are repaired. Motion is started almost immediately to prevent repeat scarring of the tendon to the sheath and overlying soft tissue, and weight-bearing should follow as soon as pain and swelling permit, usually less than one to two weeks. Return to competitive activity takes three to six months. Since tendinosis involves changes in the substance of the tendon, brisement is of no benefit. Surgery consists of cutting out scar tissue and calcification deposits within the tendon. Abnormal tissue is excised until tissue with normal appearance appears. The tendon is then repaired with suture. In older patients or when more than 50 percent of the tendon is removed, one of the other tendons at the back of the ankle is transferred to the heel bone to assist the Achilles tendon with strength as well as provide better blood supply to this area.
Prevention
Although Achilles tendinitis cannot be completely prevented, the risk of developing it can be lowered. Being aware of the possible causes does help, but the risk can be greatly reduced by taking the following precautions. Getting a variety of exercise - alternating between high-impact exercises (e.g. running) and low-impact exercise (e.g. swimming) can help, as it means there are days when the Achilles tendon is under less tension. Limit certain exercises - doing too much hill running, for example, can put excessive strain on the Achilles tendon. Wearing the correct shoes and replacing them when worn - making sure they support the arch and protect the heel will create less tension in the tendon. Using arch supports inside the shoe, if the shoe is in good condition but doesn't provide the required arch support this is a cheaper (and possibly more effective) alternative to replacing the shoe completely. Stretching, doing this before and after exercising helps to keep the Achilles tendon flexible, which means less chance of tendinitis developing. There is no harm in stretching every day (even on days of rest), as this will only further improve flexibility. Gradually increasing the intensity of a workout - Achilles tendinitis can occur when the tendon is suddenly put under too much strain, warming up and increasing the level of activity gradually gives your muscles time to loosen up and puts less pressure on the tendon.
Achilles tendinitis is an inflammation (swelling) of the tendon, which usually occurs as a result of overuse injury. Basketball players are the most susceptible to Achilles tendinitis because of the frequent jumping. Any activity requiring a constant pushing off the foot, such as running or dancing, may result in swelling of the tendon.
Causes
Poorly conditioned athletes are at the highest risk for developing Achilles tendonitis, also sometimes called Achilles tendinitis. Participating in activities that involve sudden stops and starts and repetitive jumping (e.g., basketball, tennis, dancing) increases the risk for the condition. It often develops following sudden changes in activity level, training on poor surfaces, or wearing inappropriate footwear. Achilles tendonitis may be caused by a single incident of overstressing the tendon, or it may result from a series of stresses that produce small tears over time (overuse). Patients who develop arthritis in the heel have an increased risk for developing Achilles tendonitis. This occurs more often in people who middle aged and older. The condition also may develop in people who exercise infrequently and in those who are just beginning an exercise program, because inactive muscles and tendons have little flexibility because of inactivity. It is important for people who are just starting to exercise to stretch properly, start slowly, and increase gradually. In some cases, a congenital (i.e., present at birth) condition causes Achilles tendonitis. Typically, this is due to abnormal rotation of the foot and leg (pronation), which causes the arch of the foot to flatten and the leg to twist more than normal.
Symptoms
Common symptoms of Achilles tendinitis include weakness in the leg, slight pain above the heel in the lower leg after activity, feeling of stiffness in the leg that usually appears in the morning and lessens throughout the day, bad pain the day after exercising, pain as you climb stairs or go uphill, swelling in the area of the Achilles tendon, creaking or cracking noise when you press on the Achilles tendon.
Diagnosis
Studies such as x-rays and MRIs are not usually needed to make the diagnosis of tendonitis. While they are not needed for diagnosis of tendonitis, x-rays may be performed to ensure there is no other problem, such as a fracture, that could be causing the symptoms of pain and swelling. X-rays may show evidence of swelling around the tendon. MRIs are also good tests identify swelling, and will show evidence of tendonitis. However, these tests are not usually needed to confirm the diagnosis; MRIs are usually only performed if there is a suspicion of another problem that could be causing the symptoms. Once the diagnosis of tendonitis is confirmed, the next step is to proceed with appropriate treatment. Treatment depends on the specific type of tendonitis. Once the specific diagnosis is confirmed, the appropriate treatment of tendonitis can be initiated.
Nonsurgical Treatment
In most cases, nonsurgical treatment options will provide pain relief, although it may take a few months for symptoms to completely subside. Even with early treatment, the pain may last longer than 3 months. If you have had pain for several months before seeking treatment, it may take 6 months before treatment methods take effect. The first step in reducing pain is to decrease or even stop the activities that make the pain worse. If you regularly do high-impact exercises (such as running), switching to low-impact activities will put less stress on the Achilles tendon. Cross-training activities such as biking, elliptical exercise, and swimming are low-impact options to help you stay active. Placing ice on the most painful area of the Achilles tendon is helpful and can be done as needed throughout the day. This can be done for up to 20 minutes and should be stopped earlier if the skin becomes numb. A foam cup filled with water and then frozen creates a simple, reusable ice pack. After the water has frozen in the cup, tear off the rim of the cup. Then rub the ice on the Achilles tendon. With repeated use, a groove that fits the Achilles tendon will appear, creating a "custom-fit" ice pack. Drugs such as ibuprofen and naproxen reduce pain and swelling. They do not, however, reduce the thickening of the degenerated tendon. Using the medication for more than 1 month should be reviewed with your primary care doctor. The following exercise can help to strengthen the calf muscles and reduce stress on the Achilles tendon. Lean forward against a wall with one knee straight and the heel on the ground. Place the other leg in front, with the knee bent. To stretch the calf muscles and the heel cord, push your hips toward the wall in a controlled fashion. Hold the position for 10 seconds and relax. Repeat this exercise 20 times for each foot. A strong pull in the calf should be felt during the stretch. Physical therapy is very helpful in treating Achilles tendinitis. It has proven to work better for noninsertional tendinitis than for insertional tendinitis. Eccentric strengthening is defined as contracting (tightening) a muscle while it is getting longer. Eccentric strengthening exercises can cause damage to the Achilles tendon if they are not done correctly. At first, they should be performed under the supervision of a physical therapist. Once mastered with a therapist, the exercises can then be done at home. These exercises may cause some discomfort, however, it should not be unbearable. Stand at the edge of a stair, or a raised platform that is stable, with just the front half of your foot on the stair. This position will allow your heel to move up and down without hitting the stair. Care must be taken to ensure that you are balanced correctly to prevent falling and injury. Be sure to hold onto a railing to help you balance. Lift your heels off the ground then slowly lower your heels to the lowest point possible. Repeat this step 20 times. This exercise should be done in a slow, controlled fashion. Rapid movement can create the risk of damage to the tendon. As the pain improves, you can increase the difficulty level of the exercise by holding a small weight in each hand. This exercise is performed similarly to the bilateral heel drop, except that all your weight is focused on one leg. This should be done only after the bilateral heel drop has been mastered. Cortisone, a type of steroid, is a powerful anti-inflammatory medication. Cortisone injections into the Achilles tendon are rarely recommended because they can cause the tendon to rupture (tear).
Surgical Treatment
For paratenonitis, a technique called brisement is an option. Local anesthetic is injected into the space between the tendon and its surrounding sheath to break up scar tissue. This can be beneficial in earlier stages of the problem 30 to 50 percent of the time, but may need to be repeated two to three times. Surgery consists of cutting out the surrounding thickened and scarred sheath. The tendon itself is also explored and any split tears within the tendon are repaired. Motion is started almost immediately to prevent repeat scarring of the tendon to the sheath and overlying soft tissue, and weight-bearing should follow as soon as pain and swelling permit, usually less than one to two weeks. Return to competitive activity takes three to six months. Since tendinosis involves changes in the substance of the tendon, brisement is of no benefit. Surgery consists of cutting out scar tissue and calcification deposits within the tendon. Abnormal tissue is excised until tissue with normal appearance appears. The tendon is then repaired with suture. In older patients or when more than 50 percent of the tendon is removed, one of the other tendons at the back of the ankle is transferred to the heel bone to assist the Achilles tendon with strength as well as provide better blood supply to this area.
Prevention
Although Achilles tendinitis cannot be completely prevented, the risk of developing it can be lowered. Being aware of the possible causes does help, but the risk can be greatly reduced by taking the following precautions. Getting a variety of exercise - alternating between high-impact exercises (e.g. running) and low-impact exercise (e.g. swimming) can help, as it means there are days when the Achilles tendon is under less tension. Limit certain exercises - doing too much hill running, for example, can put excessive strain on the Achilles tendon. Wearing the correct shoes and replacing them when worn - making sure they support the arch and protect the heel will create less tension in the tendon. Using arch supports inside the shoe, if the shoe is in good condition but doesn't provide the required arch support this is a cheaper (and possibly more effective) alternative to replacing the shoe completely. Stretching, doing this before and after exercising helps to keep the Achilles tendon flexible, which means less chance of tendinitis developing. There is no harm in stretching every day (even on days of rest), as this will only further improve flexibility. Gradually increasing the intensity of a workout - Achilles tendinitis can occur when the tendon is suddenly put under too much strain, warming up and increasing the level of activity gradually gives your muscles time to loosen up and puts less pressure on the tendon.